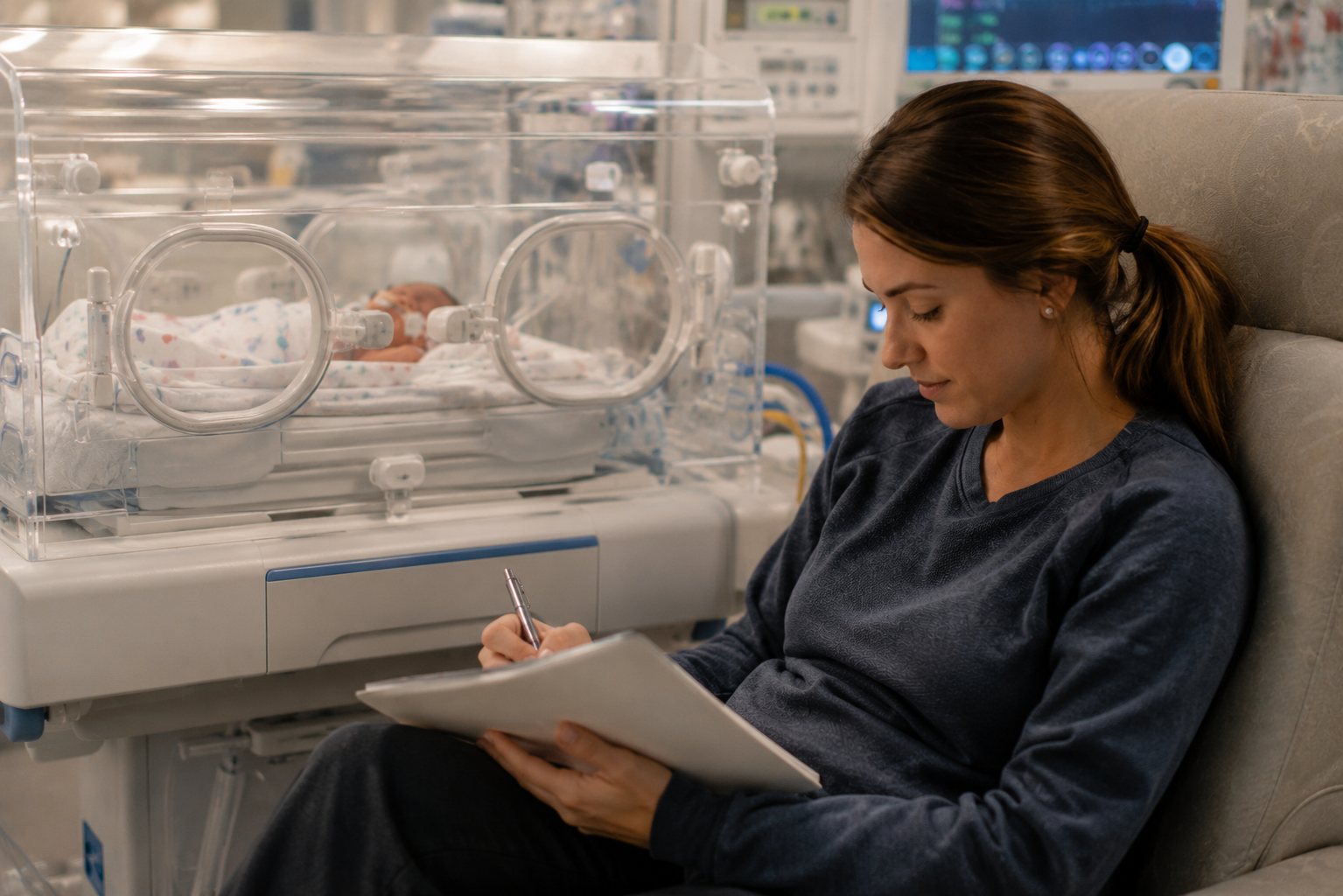
Navigate NICU emotions with self-care tips & support. Reach out for resources to help you and your family during this journey.

Discover the essential mental health and logistical support NICU families need after discharge, featuring expert insights and research-backed data from Miracle Babies.

Maternal Mental Health is Essential Care - By Stacy Cowart